搜尋
共有:找到一項結果。

李懿軒醫師
.jpg)
醫師代號:03158
專長
- 腹部急症手術
- 一般消化外科手術
- 各式腸胃道造口手術
現職
- 佛教慈濟醫療財團法人花蓮慈濟醫院一般外科主治醫師
學歷
- 慈濟大學醫學系
經歷
- 花蓮慈濟醫院外科部一般外科總住院醫師
期刊發表
1. Previous non-hepatectomy abdominal surgery did not increase the difficulty in laparoscopic hepatectomy for hepatocellular carcinoma: A case–control study in consecutive 100 patients; Tzu Chi Medical Journa, Yi-hsuan Lee, Hsiu-Hsien Lin, Tsai-Ling Kuo, Ming-Che Lee, Yen-Cheng Chen
2. Laparoscopic Hepatectomy is a Feasible and Safe Choice for Primary Hepatocellular Carcinoma; Surgery Insights; 2022; Yi-Hsuan Lee, Yu-Ting Huang, Tsai-Ling Kuo, Ming-Che Lee, Yen-Cheng Chen
刀治病態肥胖
刀治病態肥胖
淺談減重及代謝手術
肥胖是百病之源,許多慢性病包括糖尿病、高血壓、心臟病、腦血管病變、睡眠呼吸中止症、退化性關節炎等常伴隨肥胖而來,不僅對個人的健康影響甚鉅,也造成龐大的社會及醫療財政負擔。
減重手術
以下介紹三種為美國FDA通過合法且常見的減重術式。各種手術均有其優缺點,需經醫師專業評估後,選擇出最合適的術式。
胃束帶(Laparoscopic Adjustable Gastric Banding)
經由腹腔鏡手術將可結節式的環狀術帶,束於胃上部,將胃分隔成兩個部分。因上胃儲存食物空間減少,患者易有飽足感,而達到控制進食量之目的。胃束帶手術減重效果較為緩慢,術後2-3年可減去超重體重的50%, 住院天數約2天。
胃束帶手術以限制患者熱量的攝取來控制減輕體重,因此不適合愛好攝取高熱量液態食物(如冰淇淋、巧克力等甜食)的患者。
胃繞道(Laparoscopic Roux-en-Y gastric bypass)
胃繞道屬於風險較高且手術過程複雜的術式,主要是將胃分成大小胃囊,再將小腸繞過150cm與小胃囊相接,經由同時限制進食胃容量及減少腸吸收長度,達到減重之效果。此術式目前被視為治療第二型糖尿病的黃金標準手術,且減重效果最佳。術後12~18個月可達到最大的成效,術後一年可減去過重體重的70%,住院天數約5-7天。
胃繞道後食物直接進入空腸內,可能會引起傾倒症候群,另外,除了降低熱量的吸收外,維生素的吸收也會減少,故術後長期需補充B12、鈣及鐵等維生素,避免維生素攝取不足之現象。
袖狀胃切除(胃縮小)(Laparoscopic sleeve gastrectomy)
利用腹腔鏡手術將胃部分切除,保留下1/4的胃(約100 cc左右),以縮小胃容積來減少進食量,且部分胃切除後饑餓激素(Ghrelin)的分泌會下降,患者不容易感到飢餓。胃縮小手術效果雖然不如胃繞道手術,但相差不大,手術安全性較好,術後併發症少,為減重手術的最佳選擇。術後12~18個月可達到最大的成效,平均減去過重體重的60%,住院天數約5天。
袖狀胃切除手術可能會加重胃潰瘍或胃食道逆流的症狀,因此不適合有胃潰瘍或嚴重胃食道逆流的患者。
【一般外科】介紹
緣起
 由於上人有感於「貧因病起,病由貧生」,尤以花東部地區地形狹長,山川重阻,交通不便,缺乏完善的醫療設施。在上人思索:生命尊嚴,平等無異;為服務東部病患,解決貧困的根源,乃於六十八年間,毅然發心建院。在多方的努力下,於民國七十五年八月十七日慈濟醫院正式落成啟用,經多年之積極經營,規模已由當年的二百五十床增加至目前的九百二十六床,同時升格為醫學中心。在這期間,一般外科無論在教學、研究或臨床服務各方面均努力提升水準。目前一般外科共有普通病房五十四床,加護病房十五床,除提供一般外科所有的臨床服務外,亦是東部唯一能提供器官移植醫療的醫院。
由於上人有感於「貧因病起,病由貧生」,尤以花東部地區地形狹長,山川重阻,交通不便,缺乏完善的醫療設施。在上人思索:生命尊嚴,平等無異;為服務東部病患,解決貧困的根源,乃於六十八年間,毅然發心建院。在多方的努力下,於民國七十五年八月十七日慈濟醫院正式落成啟用,經多年之積極經營,規模已由當年的二百五十床增加至目前的九百二十六床,同時升格為醫學中心。在這期間,一般外科無論在教學、研究或臨床服務各方面均努力提升水準。目前一般外科共有普通病房五十四床,加護病房十五床,除提供一般外科所有的臨床服務外,亦是東部唯一能提供器官移植醫療的醫院。
◎ 胰臟癌腹腔鏡手術-90歲爺爺挺過來
胰臟癌腹腔鏡手術 90歲爺爺挺過來

杭爺爺(左三)出院當天,陳言丞主任(左二)與一般外科照護團隊準備蛋糕祝福。
你有上腹痛、背痛、黃疸、體重減輕,甚至拉肚子的症狀嗎?花蓮慈濟醫院外科主任陳言丞表示,若有請盡快到醫院腸胃肝膽科接受專業醫師評估,安排進一步檢查,因為這些都是胰臟癌細胞持續擴大後的症狀。 陳言丞指出,胰臟位在後腹腔,時常會被忽略,而且早期病變症狀不是很明顯。根據統計,每年胰臟癌死亡個案數佔新診斷個案數約近九成,且胰臟癌中以腺癌最多,約有七成好發在胰臟頭部,二成在胰臟體部,一成在尾部。
他表示,如果癌症是發生於胰頭,則癌細胞有可能侵犯到膽管而導致膽汁無法暢流至十二指腸,這時病患會出現皮膚發黃、眼角膜發黃、尿液呈現深茶色或皮膚會有發癢的情形,嚴重者甚至會有發燒或畏寒等膽管炎的症狀,若動手術通常採用胰頭十二指腸切除術(Laparoscopic Pancreaticoduodenectomy, Whipple Operation)。
高齡長者也能動手術
目前在臺灣只有少數醫院成功開展十二指腸切除手術幫助病患。為降低相關手術風險,陳言丞自二年前起以腹腔鏡執行胰頭,使用腹腔鏡可以將重要的手術視野放大約五至十倍於大螢幕上、各種組織及血管的辨識度大大提升,相比傳統的開腹手術,傷口小、出血少、傷害也能盡量減輕,大大放寬適用的年齡範圍,讓許多高齡長者也能接受這樣高難度的手術。
近期有一位九十歲的杭爺爺,平時三餐飲食正常,還有運動習慣,完全沒有什麼不舒服的症狀,直到今年農曆春節過後,孫子們都覺得他明顯變瘦且眼白與皮膚發黃、且有全身發癢的狀況,他也覺得自己較往常容易腹瀉的症狀,便在女兒的建議下,來到花蓮慈濟醫院腸胃內科就醫檢查,發現為胰臟頭部腫瘤造成膽管與胰管阻塞,於是接受陳言丞主任手術治療。
術後第二天就到一般病房
術後杭爺爺表示,手術後第二天就到一般病房了,而且一點都不痛,現在健走運動也都不會喘,感覺又重新活過來了。杭爺爺的女兒也表示,真的很謝謝陳言丞主任跟醫護團隊,從頭到尾的治療都很仔細,讓高齡的爸爸在治療過程中都很順利。
陳言丞醫師提醒,儘管胰臟癌好發年齡在六七十歲,一般來說年紀超過四十歲,出現類似上述胰臟癌症狀且不明原因時,最好盡快到醫院腸胃肝膽科接受專業醫師評估,進而安排進一步可能之檢查,如腹部超音波、電腦斷層掃描、核磁共振等,有助於釐清病因,及早治療。而平日少糖、少油、少鹽、高纖維質飲食,不僅可以防治高血壓、高血脂、高血糖等疾病,再加上遠離菸和酒,以及養成運動的習慣,時下健康的生活型態也是防癌的不變法則。
實習記者許嫚修/2020年03月29日 更生日報報導
腎臟移植
本院於1995年成立器官移植小組,1997年執行首例屍體腎臟移植,2000年完成第一例活體腎臟移植,截至2013年底已完成114例屍體腎臟移植,31例活體腎臟移植,共145例【表一】。
表一、年度移植案例數
| 年 度 | 屍腎移植 | 活腎移植 |
| 2000-2004 | 31 | 8 |
| 2005 | 12 | 3 |
| 2006 | 3 | 2 |
| 2007 | 13 | 4 |
| 2008 | 16 | 5 |
| 2009 | 5 | 2 |
| 2010 | 13 | 4 |
| 2011 | 9 | 0 |
| 2012 | 7 | 1 |
| 2013 | 5 | 2 |
| 總 計 | 114 | 31 |
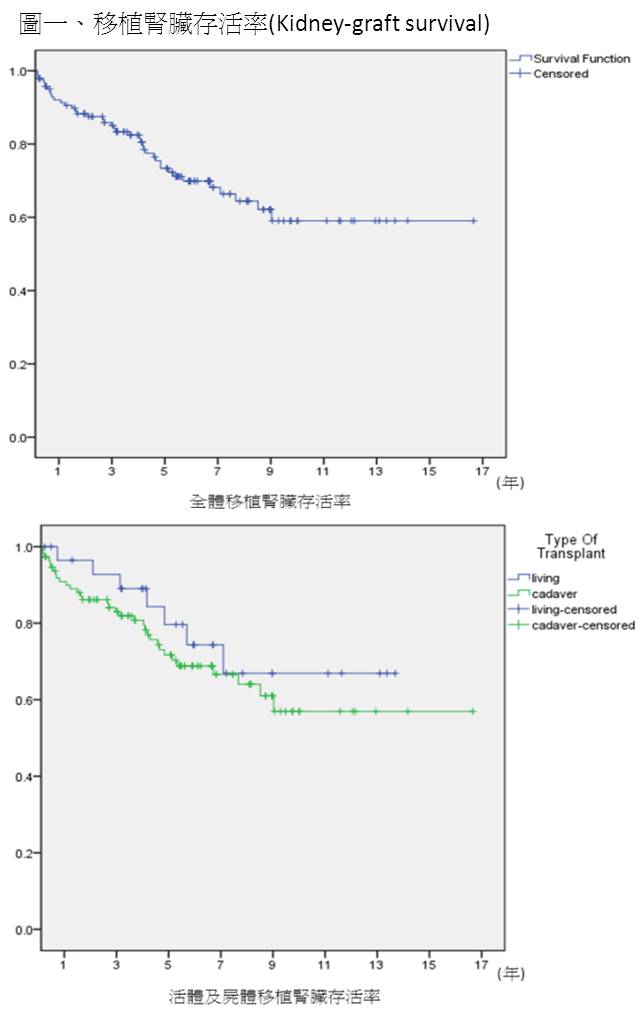
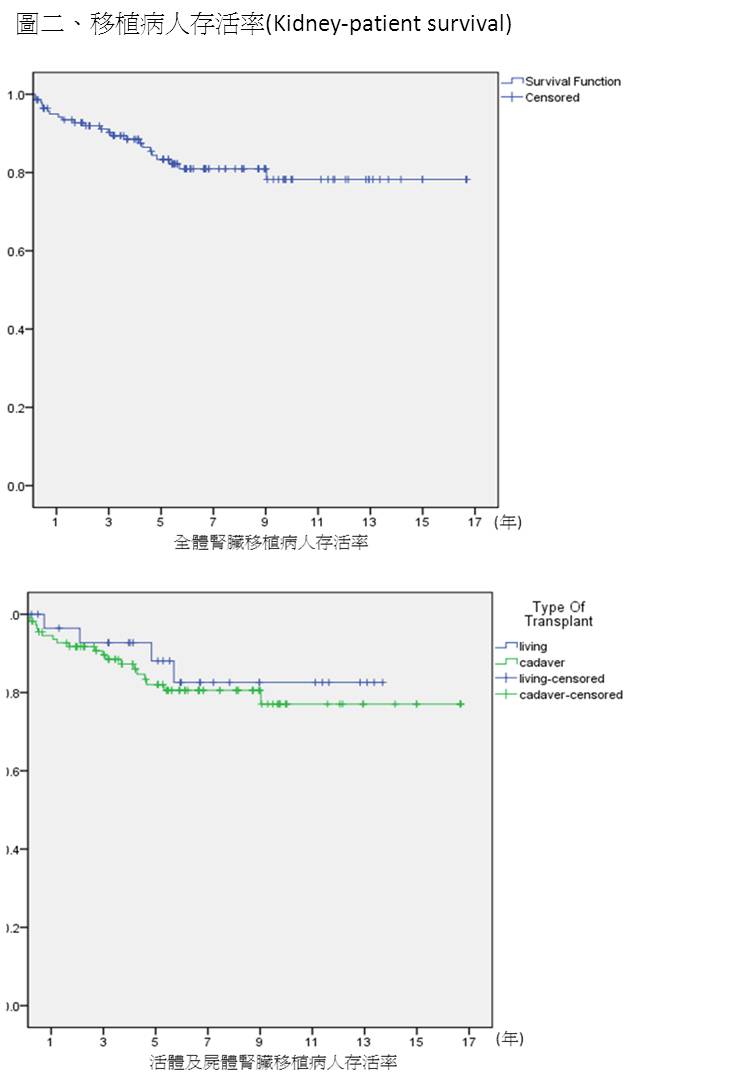
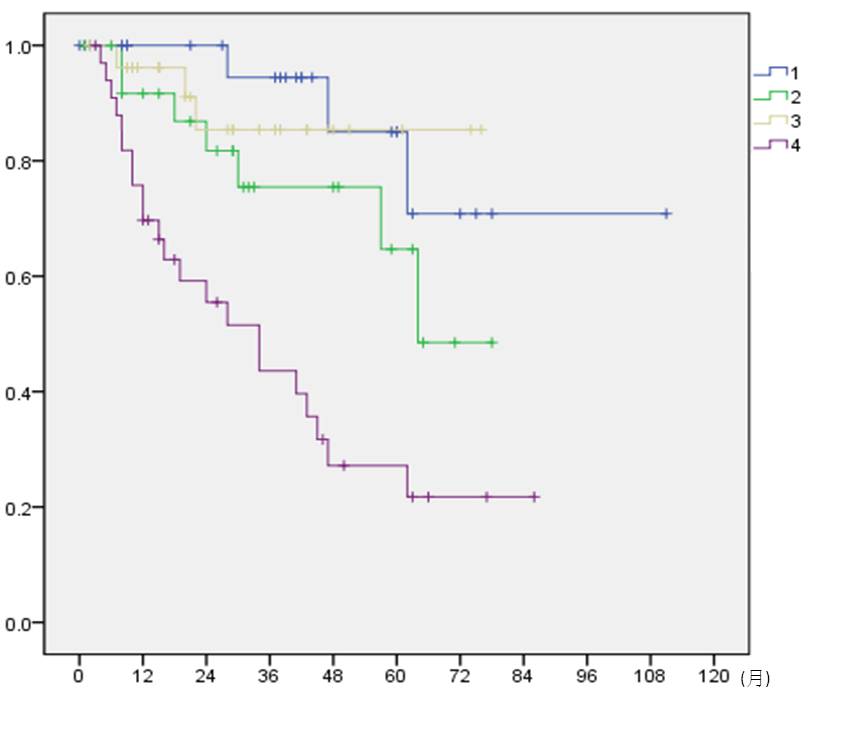
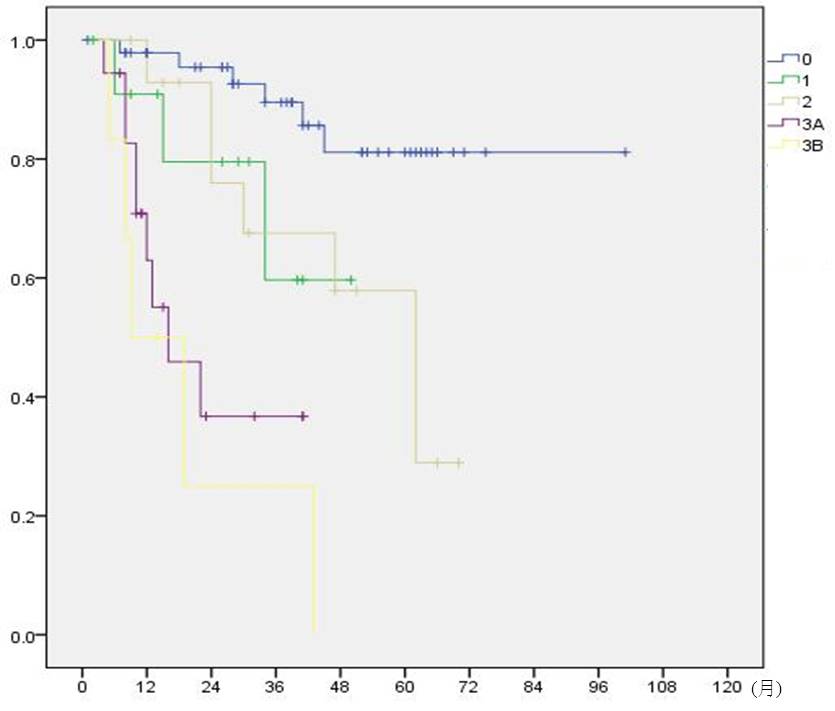
接受腎臟移植病患平均年齡46.16歲,其中男性占53.5%,平均追蹤時間為5.96年,全體3年移植腎臟存活率(Kidney-graft survival)為84.2%【表二、圖一】,3年腎臟移植病患存活率(Kidney-patient survival)為89.4%【表三、圖二】。
表二、移植腎臟存活率(Kidney-graft survival)
| 1年 | 3年 | 5年 | 7年 | 10年 | |
| 全體 | 0.913 | 0.842 | 0.734 | 0.664 | 0.590 |
| 活體捐贈移植 | 0.964 | 0.927 | 0.796 | 0.669 | 0.669 |
| 屍體捐贈移植 | 0.899 | 0.819 | 0.717 | 0.569 | 0.569 |
表三、腎臟移植病人存活率(Kidney-patient survival)
| 1年 | 3年 | 5年 | 7年 | 10年 | |
| 全體 | 0.942 | 0.894 | 0.833 | 0.809 | 0.782 |
| 活體捐贈移植 | 0.964 | 0.927 | 0.881 | 0.826 | 0.826 |
| 屍體捐贈移植 | 0.936 | 0.885 | 0.820 | 0.806 | 0.771 |
語音掛號說明
![]()
. 操作說明:
1.請依各院語音掛號號碼撥號。
2.使用國語發音請按1,使用台語發音請按2,使用英語發音請按3。
3.本院電話語音的功能有:(1)預約掛號、(2)查詢掛號、(3)取消掛號、(4)快速掛號、(5)查詢 醫師排班表、(6)本院公告、(7)系統使用說明。
4.輸入病歷號碼:
(1) 複診病患為身份證字號數字部分,口口口口口口口口口 共9位。
(2) 初診病患為身份證字號,口口 ─ 口口口口口口口口口 共11位。
( 前二位為英文字母代碼,後九位為數字部分。)
(3) 若您的病歷號碼非身分證字號,則請輸入本院掛號證上之數字,輸入結束並按「#」鍵。
(4) 英文字母代碼對照表。
|
A |
B
|
C |
D |
E |
F |
G |
H |
I |
J |
K |
L |
M |
|
01 |
02 |
03 |
04 |
05 |
06 |
07 |
08 |
09 |
10 |
11 |
12 |
13 |
|
N |
O |
P |
Q |
R |
S |
T |
U |
V |
W |
X |
Y |
Z |
|
14 |
15 |
16 |
17 |
18 |
19 |
20 |
21 |
22 |
23 |
24 |
25 |
26 |
6.輸入看診時段:上午門診請按1 、下午門診請按 2、夜間門診請按3 。
7.輸入看診醫師代號:請參照門診表上醫師姓名下方之 醫師代號。 ( 如陳英和醫師,醫師代號為 0901)
8.預約掛號開放時間為一個月內(臺中慈院,三十五日內)。
減重術後的飲食
減重術後的飲食
對於即將接受減重手術的患者,營養師會給予完整的術前及術後營養評估,而在手術後也需進行階段式的飲食調整。依據不同手術方式,調整進食階段有所不同,切勿自行調整,造成不適感及減重效果變差。術後胃容量縮小、腸胃道吸收減弱,如有相關營養問題,需充分與醫師及營養師討論,才能健康享瘦.....<詳見全文>
(轉載人醫心傳第147期,文/紀凱勻 花蓮慈濟醫院營養師)

◎ 「胰腸所願」腹腔鏡胰頭十二指腸腫瘤手術
胰臟是兼具內分泌及外分泌功能的消化器官,因位於人體後腹腔深處,與許多器官連結,以致於手術難度高,胰臟癌中的腹腔鏡胰頭十二指腸切除手術可謂外科術式中最難攻項的「聖母峰」等級手術,但治療成效佳,且病人復原期短。
胰臟腫瘤早期症狀不明顯,四十歲以上若陸續出現上腹悶脹疼痛、背痛、嘔吐感、胃口變差、體重減輕、黃疸、腹瀉等症狀,請盡快檢查以掃除胰臟腫瘤的疑慮。


文/游繡華、黃思齊、江家瑜
談到胰臟癌,許多人會想到前蘋果電腦執行長賈伯斯(Steve Jobs)。而死於胰臟癌的名人還包括世界男高音帕華洛帝、臺灣的音樂人梁弘志、洪一峰、資深媒體人傅達仁……,以及臺灣醫界最年輕的醫療奉獻獎得主,自費買船、學開船,到離島行醫的侯武忠醫師,他們幾乎都是在發現罹患胰臟癌後一年左右就撒手人寰。
胰臟癌預後差 癌中之王
胰臟癌是自胰臟細胞生長出來的惡性腫瘤,雖然不常見,根據國民健康署的統計,二○一六年,胰臟癌發生個案數占全部惡性腫瘤發生個案數的2.08%,發生率排名是第十三位。而同年胰臟癌死亡人數占全部癌症死亡人數的4.18%;在近幾年的十大癌症死亡率排名中幾乎是於男性第八位、女性第五位。
儘管肺癌和肝癌的死亡率較高,但因為胰臟位在後腹腔,時常會被忽略,而且發生病變的時候,往往又因症狀不是很明顯,等到病人意識到疼痛就醫時,癌細胞大多已侵犯到鄰近器官已發展到晚期,也因此約有八、九成的胰臟癌病人,發現時都已無法手術治療;五年的存活率都低於5%,可以說是預後最差的癌症;而被稱為「癌中之王」。

胰臟位置在人體的後腹腔深處,與胃、十二指腸、空腸、膽道、脾等都有關連,使得相關疾病的手術困難度高。
「天下第一吻」
胰臟手術吻合難度高
胰臟癌中以腺癌最多,源自胰外分泌腺體,胰臟癌約有七成好發在胰頭部,二成在胰臟體部,一成在尾部。在治療上,化學治療是晚期胰臟癌的主要治療方式,如果胰臟癌尚能接受手術時,醫師都會建議病人以手術治療為優先,這是存活的最佳機會。如果是胰頭癌,手術方式較複雜,通常是採用胰頭十二指腸切除術。
空腸是整條小腸的中間部分,在十二指腸與迴腸之間。
家住花蓮市的林先生,今年七十歲,在朋友眼中是一位很重視養生的歐吉桑,不僅日常三餐飲食、生活作息正常,更有固定運動的習慣,因此在就醫檢查之前,沒有明顯不舒服的症狀。只是在二月間農曆新年過後不久,剛好是太極拳老師的生日,於是社團好友便相約餐敘為老師慶生,朋友們一見面都覺得他明顯變瘦,建議他去醫院做個檢查。
林先生說,加上他也覺得自己有比往常容易拉肚子的症狀,便到花蓮慈濟醫院腸胃內科就醫檢查,結果一掃超音波,先是發現他膽管有阻塞,進而抽血檢查,癌症指數偏高,再進一步做超音波檢查確診胰臟癌後,便轉由一般外科主任陳言丞手術治療。
陳言丞主任說,因為位置在腹腔深處的胰臟,與胃、十二指腸、空腸、膽道、脾等都有關連,使相關疾病的手術相對困難,其中以「胰十二指腸切除手術」困難度更高。自一九三五年以來,這術式一直是治療胰頭腫瘤、膽管中下段、壺腹部,與十二指腸腫瘤的標準術式;切除臟器包括胰臟頭部十二指腸、肝外膽管、部分的胃與小腸等器官,甚至還需要做血管的切除與吻合,在切除後仍需進行精密且複雜的重建手術,包括胰腸、膽腸與胃腸吻合,是手術成敗的關鍵,臺灣醫界更以「天下第一吻」來形容胰臟吻合的高困難度與重要性。

胰頭十二指腸結構複雜,「腹腔鏡胰頭十二指腸切除手術」難度被喻為現代外科的「聖母峰」。虛線表示胰頭切除部位。

胰頭十二指腸手術切除後,需進行精密且複雜的重建手術,包括胰腸、膽腸與胃腸吻合,臺灣醫界以「天下第一吻」來形容胰臟吻合的高困難度與重要性。
腹腔鏡胰頭十二指腸切除術
縮短術後復原時間
由於傳統開腹手術, 傷口大、風險高,術後併發症多;為了降低手術風險,陳言丞主任自二年前開始以腹腔鏡做胰頭十二指腸切除手術。這項被喻為現代外科聖母峰的「腹腔鏡胰頭十二指腸切除術(Laparoscopic Pancreaticoduodenectomy, Whipple Operation)」,目前在臺灣只有少數醫院成功開展這項手術幫助病人。腹腔鏡手術相比傳統開腹手術有著許多不可替代的優勢,如減輕術後發炎反應,對病人免疫力的影響更小。
陳言丞主任說,執行腹腔鏡胰頭十二指腸切除手術,透過腹腔鏡五到十倍的放大視野,有利於重要組織器官的辨識,即使是位在腹腔深處的胰臟,且可更清晰的裸露血管,在清除淋巴腺與周圍結締組織及減少術中出血等方面,更勝於傳統開腹手術;因為傷口小,出血少,感染風險低,也大大縮短病人復原的時間。
林先生在手術後第二天,就自加護病房轉到一般病房了,而且傷口竟然一點都不痛。他說,真的很感謝陳言丞主任跟醫護團隊,從頭到尾的治療都很仔細,一開始先解決他的膽管阻塞問題,等身體狀況穩定之後,接著以腹腔鏡手術切除胰臟腫瘤。他當時聽說這個刀很難,要開很久,還有點小擔心,沒想到只住了一天加護病房後就跟沒事了一樣,現在健走運動也都不會喘,感覺又重新活過來了。

病人以腹腔鏡進行胰頭十二指腸切除手術,傷口小、復原速度佳。

相較於傳統術式,腹腔鏡手術有助於病人盡快恢復。圖/一般外科提供
胰臟癌初期應積極治療
九十九歲也成功
同樣是做腹腔鏡胰頭十二指腸切除手術治療胰臟癌的黃女士,她是慈濟志工,談起去年從診斷到治療過程,她要特別感謝小兒部的朱紹盈醫師和家庭醫學科黃亮凱醫師。黃女士除了是骨髓關懷小組志工,也是醫療志工,每年都會協助慈院團隊執行花蓮縣各校學童健檢,去年暑假期間,這兩位醫師一見到她,就直說她怎麼變更瘦了,請她要注意健康狀況。但因她本身就是身形較瘦,精神也不錯,根本不會覺得自己生病了。
黃女士說,儘管黃亮凱醫師催促她一定要檢查,但她就是不怎麼在意,幸好黃醫師沒有放棄,反而仔細的研究她的病歷,發現多年前曾檢查出她的肝臟有血管瘤,藉此強烈建議她務必要做超音波檢查,看一看血管瘤變化。就這樣,她終於「勉強」去檢查看看。經過超音波檢查,發現肝內膽管擴張,於是轉診給肝膽腸胃科林振雄醫師深入檢查,確診為胰臟癌,便建議她接受手術治療。
黃女士與先生討論後,決定要以自然療法對抗病魔,不接受手術治療。黃亮凱醫師得知後,認為黃女士是癌症初期,沒有轉移的現象,有很高的機率可以痊癒,所以極力勸她一定要開刀接受治療,並建議她找陳言丞主任。黃醫師說,因為他的父親也是罹患胰臟癌,當時是由陳言丞主任為父親做移除腫瘤手術,他非常相信「學長的能力」(同為慈濟大學醫學系),認為「師姑可以放心接受手術治療」。
「慈濟人最怕不能做慈濟事!」黃女士說,當時黃亮凱醫師跟許多醫護同仁、志工都很關心她,一開始沒有特別放在心上,一心只想繼續開心做志工,直到黃醫師問她「師姑,你打算志工只做到今年嗎?」回想起來,這句話真的有敲打到她的心,沒想到,隔沒幾天在醫院做志工時,又遇到精舍師父,「師父故意擺出怒目金剛的架式,勸我將身體交給醫師,好好聽醫師的話接受治療。」關心她的林振雄醫師遇到她也提起佛法「人身難得今已得」,勸她接受手術治療的話還沒說完,她就回答:「我知道林醫師你要說什麼,不用多說了,我這就乖乖去回診!」說完,她轉個彎就直接到陳言丞主任的門診報到。
她是在去年(二○一八)九月經陳言丞主任以腹腔鏡手術後,在術後第四天,就下床走路復健。三、四個月後,她又開始做志工了,同時也持續在中醫科繼續針灸調養身體。今年(二○一九)五月,她參加佛誕節慈濟浴佛大典,彩排供花燈時站了四個半小時,也不覺得累;她很感恩醫療團隊,讓已七十歲的她恢復健康的身體,繼續做志工。
「這項手術,我們開過年紀最大的病人是九十九歲!」陳言丞指出,兩年來,這項高難度的腹腔鏡手術,已成功幫助二十個病人順利出院並恢復良好。通常病人在術後的飲食狀態恢復較慢,主要是因為食物的消化吸收需要胃和小腸配合,所以,他也會提醒病人在術後除了配合用藥之外,還要清淡飲食,減少高蛋白、高油脂食物,以避免腹瀉;同時也要注意澱粉攝取量。
防治三高多運動 健康無癌生活
胰臟癌的致病原因目前仍不明,有胰臟癌家族史、吸菸、酗酒、習慣高油脂飲食、曾患有慢性胰臟炎,都是可能的風險因子,另外,某些洗衣廠或石油相關化學藥品廠的工作人員也較容易得到胰臟癌;糖尿病人罹患胰臟癌的人數也較多。
林先生和黃女士在就醫之前都有原因不明的體重明顯減輕三至四公斤以上,林先生還有拉肚子症狀。早期胰臟癌是沒有症狀的,而是隨著腫瘤漸漸擴大,才會依照腫瘤形成時在胰臟的部位變化,陸續出現上腹悶脹或疼痛、背痛、嘔吐感、胃口變差、體重減輕,黃疸或腹瀉等症狀。
醫師提醒,儘管胰臟癌好發年齡在六七十歲,一般來說年紀超過四十歲,出現類似上述胰臟癌症狀且不明原因時,最好盡快到醫院腸胃肝膽科接受腹部超音波、電腦斷層掃描、核磁共振等檢查,有助於釐清病因,進一步治療。而平日少糖、少油、少鹽、高纖維質飲食,不僅可以防治高血壓、高血脂、高血糖等疾病,再加上遠離菸和酒,以及養成運動的習慣,時下健康的生活型態也是防癌的不變法則。

林先生與黃女士特地出席花蓮慈院新聞發布會,感謝一般外科陳言丞主任及醫療團隊。左起:一般外科陳華宗醫師、外科部張睿智主任、陳培榕副院長、賴鴻緒顧問、林欣榮院長、黃女士、林先生、陳言丞主任、外科專科護理師郭綵玲、柯佳蓉、手術室李怡燕護理長、住院醫師林修賢。攝影/楊國濱
肝臟移植
本院於1995年成立器官移植小組,2003年執行首例屍體肝臟移植,2007年完成第一例活體肝臟移植,截至2013年底已完成30例屍體肝臟移植,7例活體肝臟移植,共37例【表一】。
表一、年度肝臟移植案例數
| 年 度 | 屍肝移植 | 活肝移植 |
| 2003-2004 | 6 | * |
| 2005 | 1 | * |
| 2006 | 3 | * |
| 2007 | 5 | 1 |
| 2008 | 1 | 1 |
| 2009 | 3 | 0 |
| 2010 | 4 | 3 |
| 2011 | 4 | 1 |
| 2012 | 2 | 0 |
| 2013 | 1 | 1 |
| 總 計 | 30 | 7 |
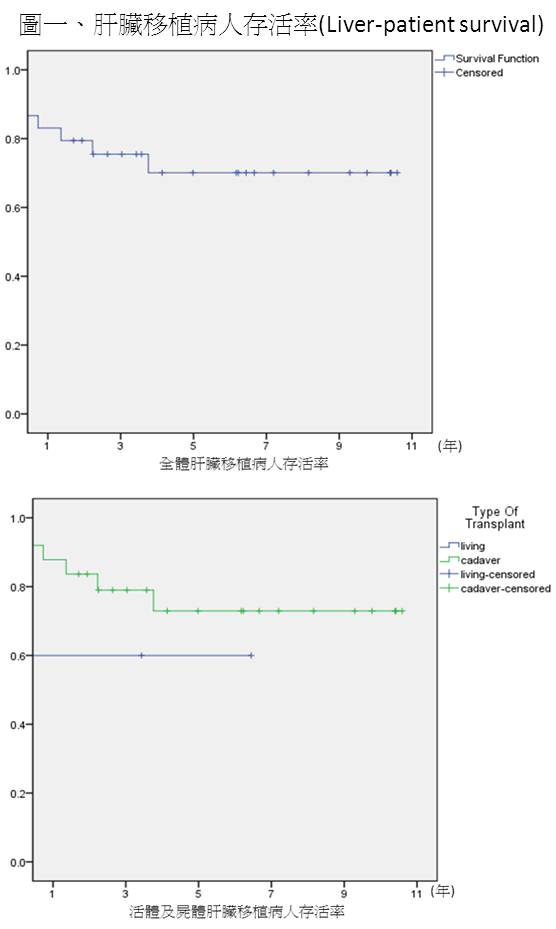
接受肝臟移植病患平均年齡49.84歲,其中男性占64.9%,平均追蹤時間為4.28年,全體3年肝臟移植病患存活率(Liver-patient survival)為75.5%【表二、圖一】。
表二、肝臟移植病人存活率(Liver-patient survival)
| 1年 | 3年 | 5年 | 7年 | 10年 | |
| 全體 | 0.831 | 0.755 | 0.701 | 0.701 | 0.701 |
| 活體捐贈移植 | 0.600 | 0.600 | 0.600 | - | - |
| 屍體捐贈移植 | 0.878 | 0.790 | 0.729 | 0.729 | 0.729 |



身體不能承受之重-告別病態性肥胖
肥胖已是現代人的重要健康課題,小時候圓滾滾的可愛,長大後如果還是一樣胖胖的,加上不忌口又缺乏運動,體重直線上升的幅度,恐怕跟年齡一樣難追回。花蓮慈濟醫院一般外科吳柏鋼醫師表示,醫學上發現身體質量指數(BMI)超過40之後,對健康已經形成危害,也稱為「病態性肥胖」,建議可考慮外科手術治療,找回健康。
胃癌
胃癌為台灣十大癌症之一,每年新診斷個案數約為3500至4000人。胃癌的治療原則以手術為主,並依照術後之病理分期來為是否接受輔助性化學治療、放射線治療、免疫療法與標靶治療之依據。
治療成果
2004至2011年,102位胃癌病患接受根治性切除手術,平均年齡為66歲,其中以男性為主,約佔65%,女性佔35%。平均追蹤時間為50個月,全體五年存活率為61%。手術後90日之死亡率為2.9%。
各分期之三年存活率分別為第一期94.4%,第二期75.4%,第三期85.4%,第四期43.6%。
局部淋巴結轉移之治療成果
依據手術後之病理報告,本院約有50%之病患有局部之淋巴結轉移,根據AJCC第七版之分類:轉移淋巴傑數目1-2為N1,3-6為N2,大於6為N3,這些病患依據分期則強烈建議需接受輔助性之化學治療與可能之放射線治療,可使存活率提升約10%。目前本院局部淋巴結轉移之胃癌病患,術後五年存活率超過50%。
總結
本院一般外科在同仁的努力下,胃癌之手術治療成果已與國內外醫學中心相當。胃癌之治療需整合一般外科,腫瘤科與放射腫瘤科之醫療團隊,對於花東地區民眾提供高品質之醫療。

大腸直腸癌
大腸直腸癌的發生是因為黏膜細胞(通嘗試息肉上的細胞)發生不正常的變化而產生失去控制的增生。而癌細胞也會經由淋巴或血液系統循環散佈到身體的其他器官,像是淋巴結、肝臟、肺臟等,這種情況稱為轉移。台灣每年新診斷之大腸直腸癌超過一萬人,與肝癌和肺癌為三大癌症。

代謝及減重手術
肥胖為導致慢性疾病的重要因素,國人十大死亡原因中,有8項與肥胖有關。除此之外,肥胖引起許多合併症,如糖尿病、高血脂、睡眠呼吸中止、心血管疾病、退化性關節炎、尿酸過高,不孕症等。過去的60年中,減重手術(bariatric surgery)治療病態性肥胖有顯著進步,包括術式更安全、器械更進,且可有效改善病患的健康狀況以及生活品質。
林修賢醫師
醫師代號:03139
專長
- 腹部急症手術
- 傳統與微創疝氣手術
- 一般消化外科手術
現職
- 佛教慈濟醫療財團法人花蓮慈濟醫院一般外科主治醫師
學歷
- 慈濟大學醫學系
經歷
- 花蓮慈濟醫院外科部一般外科總住院醫師
期刊發表
Tzu Chi Medical Journal; Serum myostatin level is a positive predictor of endothelial function measured by digital thermal monitoring of vascular reactivity in kidney transplantation patients; Hsiu-Hsien Lin, Ching-Chun Ho, Yen-Cheng Chen, Guan-Jin Ho, Bang-Gee Hsub, Ming-Che Lee